
One touch stockings of Cambridge
What does it test?
OTS is a test of executive function, spatial planning and working memory based upon the Tower of Hanoi test.
What does the task involve?
 The participant is shown two displays of coloured balls held in stockings suspended from a beam. There is a row of numbered boxes along the bottom of the screen. The participant is asked to solve problems by working out how they would move the balls in the bottom display in order to make them match the arrangements of the ball sin the top display. After some training and practice problems, the participant is asked to work out in their head how many moves the solutions to these problems require, and then touch the appropriate box at the bottom of the screen to indicate their response.
The participant is shown two displays of coloured balls held in stockings suspended from a beam. There is a row of numbered boxes along the bottom of the screen. The participant is asked to solve problems by working out how they would move the balls in the bottom display in order to make them match the arrangements of the ball sin the top display. After some training and practice problems, the participant is asked to work out in their head how many moves the solutions to these problems require, and then touch the appropriate box at the bottom of the screen to indicate their response.
Why this test
Patients with mood disorders often experience difficulties in executive functions such as planning: these can be assessed using the OTS task4.
Delayed Matching to Sample
What does it test?
DMS assesses forced choice recognition memory for non-verbalisable patterns, testing both simultaneous matching and short term visual memory.
What does the task involve?
 This test assesses visual matching ability and visual recognition memory. The participant is shown a complex visual pattern and then after a brief delay, four patterns. The participant must touch the pattern that matches the sample. In some trials the sample and the choice patterns are shown simultaneously, whereas in others there is a delay (of 0, 4 or 12 seconds) before the four choices appear.
This test assesses visual matching ability and visual recognition memory. The participant is shown a complex visual pattern and then after a brief delay, four patterns. The participant must touch the pattern that matches the sample. In some trials the sample and the choice patterns are shown simultaneously, whereas in others there is a delay (of 0, 4 or 12 seconds) before the four choices appear.
Why this test
Patients presenting with depression often show signs of forgetfulness or memory deficits. DMS is sensitive to these impairments, and can be used to assess changes over time in response to interventions.
Emotion recognition task
What does it test?
ERT measures the ability to identify emotions in facial expressions. Subjects choose between six basic emotions.
What does the task involve?
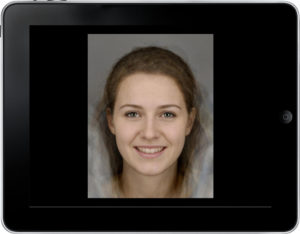 Computer morphed images derived from the facial features of real individuals each showing a specific emotion, are displayed on the screen, one at a time. Each face is displayed for 200ms and then immediately covered up, and participant must select which emotion the face displayed from 6 options.
Computer morphed images derived from the facial features of real individuals each showing a specific emotion, are displayed on the screen, one at a time. Each face is displayed for 200ms and then immediately covered up, and participant must select which emotion the face displayed from 6 options.
Why this test
Those who suffer from depression have been shown to provide more negative ratings of emotional expressions5, 6, 7. This reflects the well-known negative bias seen in depression, where positive or neutral stimuli are seen as more negative. The brief presentation encourages implicit processing, as opposed to conscious appraisal of the faces.
Spatial Working Memory
What does it test?
SWM looks at how good participants are at retaining and utilising visuospatial information. It is self-ordered and since participants must employ a strategy it also provides insight into executive function.
What does the task involve?
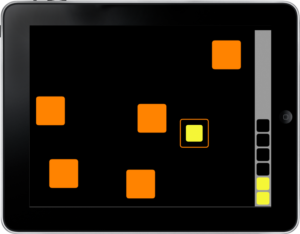 An array of coloured boxes contain tokens which participants must search for by touching the boxes. The number of boxes increases, making the task more difficult. Crucially, participants must not return to a box in which they have previously found a token.
An array of coloured boxes contain tokens which participants must search for by touching the boxes. The number of boxes increases, making the task more difficult. Crucially, participants must not return to a box in which they have previously found a token.
Why this test
Studies have shown that patients with depression have moderate impairments in working memory4. Working memory is a critical cognitive skill for a range of everyday tasks.
Rapid Visual Information Processing
What does it test?
RVP tests how well participants can sustain their visual attention and how they cope with a task requiring continuous performance.
What does the task involve?
 Single digits appear in the centre of the screen, with 100 digits being shown per minute. A panel to the right of the central square displays the target sequences which participants must respond to. When the participant detects a sequence they must press a blue button at the bottom of the screen. There are 9 target sequences per minute.
Single digits appear in the centre of the screen, with 100 digits being shown per minute. A panel to the right of the central square displays the target sequences which participants must respond to. When the participant detects a sequence they must press a blue button at the bottom of the screen. There are 9 target sequences per minute.
Why this test
RVP tests sustained attention. This cognitive domain has been found to be impaired in depression.4
Cambridge Gambling Task
What does it test?
The Cambridge Gambling Task (CGT) was developed to assess decision making and risk taking behaviour outside a learning context.
What does the task involve?
 The task requires participants to decide whether a token will be hidden behind a red box or a blue box. Participants are then asked to bet a proportion of their points to support this decision. The odds of winning or losing are made explicit in the CGT by the ratio of red to blue boxes.
The task requires participants to decide whether a token will be hidden behind a red box or a blue box. Participants are then asked to bet a proportion of their points to support this decision. The odds of winning or losing are made explicit in the CGT by the ratio of red to blue boxes.
Why this test
As information from one trial does not inform the next in the CGT, limited demands are placed on learning and working memory processes, offering a clean measure of decision-making under risk. This presents CGT as a good option for investigating the impairments in decision-making under risk typically seen in depression14.
